 Cherry tomatoes contaminated with salmonella: 92 sick and 1 dead
Cherry tomatoes contaminated with salmonella: 92 sick and 1 dead  A better coaching method can make a person grow
A better coaching method can make a person grow  What is the method to prevent diabetes in children?
What is the method to prevent diabetes in children?  What are the effective factors in causing stomach ulcers?
What are the effective factors in causing stomach ulcers?  Why do embarrassing memories seem to appear at night?
Why do embarrassing memories seem to appear at night? 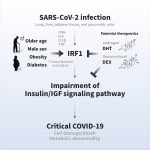 The amazing link between SARS-CoV-2 infection and newly started diabetes
The amazing link between SARS-CoV-2 infection and newly started diabetes  WHO says monkey pox is not a global emergency right now
WHO says monkey pox is not a global emergency right now  Single cell RNA sequencing uncovers new mechanisms of heart disease
Single cell RNA sequencing uncovers new mechanisms of heart disease  Hepatitis of unknown origin: 3 new deaths and 228 cases worldwide
Hepatitis of unknown origin: 3 new deaths and 228 cases worldwide 
How to treat covid patients in intensive care? A Marseille team led by Professor Laurent Papazian has made it possible to optimize the use of curare for patients in severe respiratory distress. This resuscitator followed in the footsteps of the great Claude Bernard, the first in the world to have studied curare.
Claude Bernard, one of the fathers of modern medicine, devoted years of research to deciphering the mechanism of curare. This work began at the start of his career in 1844.
At the Museum of Medical Matter in Paris, is one of the curare vials with which Claude Bernard would have worked. Its content came directly from Latin America where the Indians dipped their arrows in it before going hunting.
Dr Jean-Bernard Cazalaa, resuscitator, recounts the research of his illustrious predecessor on this poison which caused death by paralyzing the muscles of its victims : “The genius of Claude Bernard is to have tried to understand what happened after the injection of curare from the nerves to the muscles. He first tested the sensitivity. The frog used was curarized but he showed that if she was aroused, she felt it. He then showed that it did not act on the nerve since it did not act on the muscle and all the reasoning rested there. He did not have the knowledge of what was going on. was going between the nerve and the muscle, which is called the neuromuscular junction. He didn’t go any further because he died before. ”
A “heroic” remedy
Curare only blocks the control of movement without damaging either the nerve or the muscle. The heart is preserved because it does not depend on the same nervous system. Claude Bernard thus understood that death was caused by the attack on the respiratory muscles: the heart stops for lack of oxygen.
If oxygen is supplied, the heart continues to beat and the poison is eliminated from the body.
In a “popular” article on curare for the Revue des deux mondes in 1864, he explains that “the counter-poison will simply be artificial respiration”. He has an incredible vision when he concludes that “this American poison is intended to enter the class of heroic remedies.”
Use in surgery and then in intensive care
To achieve this, we will have to wait until we are able to chemically synthesize curare. Americans succeeded in 1942. The same year a Canadian anesthesiologist used it to relax the muscles of the neck and to pass the tube of intubation to the patients who were going to be operated.
Because when a person sleeps, he can move. The curare therefore supplements the anesthesia to avoid any contraction and any movement which could be dangerous during the operation. It was then adopted for exactly the same reasons in intensive care, for patients in respiratory distress for example.
Validation of curare in intensive care
It was from Marseille that a small revolution started in the use of curare in intensive care and more precisely in the North hospital, where Professor Papazian now works. At the start of his professional life, some twenty years ago, he noted with astonishment that there were no clear recommendations on the place of curare in his specialty. The only solid data comes from the operating room, which only uses it for a few hours.
Professor Laurent Papazian recounts what he implemented: “We were interested in the action in intensive care over longer periods and on patients with serious respiratory pathologies. Initially, we did a comparative scientific work with a group of patients receiving curares and a group of patients not receiving it. And so it was observed that after 48 hours, the oxygenation was better with the curares and that in addition it persisted for a few days afterwards. small trend towards reduced mortality “.
Results then confirmed
A very large study carried out with more than 20 intensive care units in 2010 confirmed this decrease in mortality with the use of curare and this from the start of treatment for a serious form of respiratory distress. When the patient cannot breathe on his own at all, the oxygen must be delivered directly to his lungs. This is the time for intubation, as Prof. Papazian explains. No movement should oppose the air flow provided by the machine.
“With regard to covid patients, patients make, as I do here, very significant respiratory efforts when they are not sufficiently sedated or curarized”describes Prof. Papazian. “And there is a stretching of the lung which aggravates the lesions, that is why they are put to rest. And so the cycles are regular, that is to say that the patient does not make any effort, since the ‘use of curares makes it possible to paralyze him completely. He is assisted 100% by the ventilator “he continues.
Mortality is therefore reduced and oxygenation takes place better, without adding additional lesions to the lungs already damaged by the massive inflammation triggered by the coronavirus. This is the reason why its use increased so much in the first wave that doctors faced a global shortage. For the moment this is no longer the case, it is to be hoped that producers have now understood that more had to be manufactured to cope with covid-19.